









Quick Links
For Patients
© Copyright 2026 American TelePhysicians. All rights reserved.
The exact cause of disease or mechanism by which it is caused is not very well known, but genetic predisposition is always there. A specific gene called HLA-B27 is present in most individuals with ankylosing spondylitis. However, HLA-B27 is not specific for the disease as it can be seen in multiple other conditions as well. And some people with ankylosing spondylitis never have this gene, meaning some acquired environmental factors might also come into play for causation.
Males are twice more likely to get affected by ankylosing spondylitis than females. The average age of clinical manifestations is 24-26 years. Clinical symptoms do not appear after 40 years, so it is less likely to develop in older adults. The disease progression in some developing countries can start as early as childhood (before the age of 16) but remains underdiagnosed.
Following clinical signs and symptoms are present in ankylosing spondylitis:
Complications of ankylosing spondylitis include:
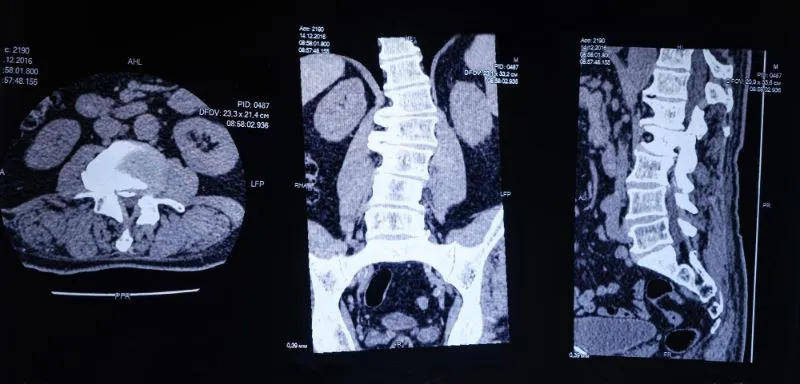
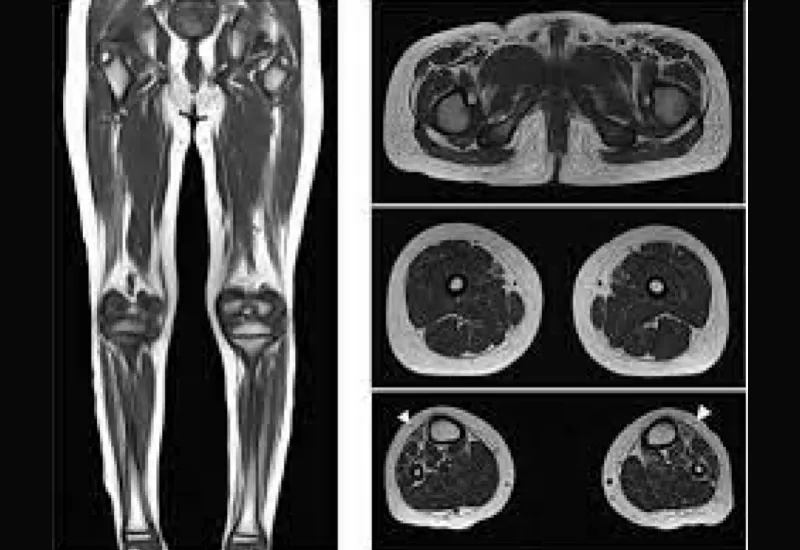
The diagnosis of ankylosing spondylitis is based upon clinical features and some radiological findings. Usually, family history, articular and extra-articular manifestations help reach the diagnosis.
Differential diagnoses of ankylosing spondylitis include:
Ankylosing spondylitis can be associated with considerable morbidity and mortality. The prognosis of ankylosing spondylitis varies greatly depending upon several factors that include:
Our clinical experts continually monitor the health and medical content posted on CURA4U, and we update our blogs and articles when new information becomes available. Last reviewed by Dr.Saad Zia on May 11, 2023.
https://link.springer.com/article/10.1007/s10067-021-05679-7




Ankylosing spondylitis is a chronic inflammatory disease that primarily affects the joints of the hip, spine, and ribs. It leads to restricted spinal mobility. The manifestations of ankylosing spondylitis vary greatly depending upon the degree of inflammation, the extent of spinal involvement, and systemic involvement. That is why it is one of the most misdiagnosed conditions. The functional impairment and work disability can affect the quality of life to a great extent. Living with the disease also has a considerable cost burden on an individual.