










Quick Links
For Patients
© Copyright 2026 American TelePhysicians. All rights reserved.
Inflammation of the gall bladder can be due to many causes, of which the most common is the obstruction of the gall bladder neck or the cystic duct. The following are the factors contributing to it:
All of the above factors lead to blockage, ultimately causing the release of various toxins and hence inflammation of the gallbladder.
According to the duration of the disease, Cholecystitis can be of two types.
Acute Cholecystitis can present typically with the following features:
Chronic Cholecystitis presents with recurrent upper abdominal pain, mostly at night and after meals.
It occurs commonly in females as compared to males, and the following are the factors that increase the risks of developing cholecystitis:
Other less common factors are gallbladder tumors and any severe systemic disease.
The diagnosis of cholecystitis is mainly clinical, but to confirm it, your healthcare provider may order some specific lab investigations after conducting a proper physical examination of the abdomen and taking the patient's history. On review, right abdominal tenderness (Pain on touching) and rigidity may be found. Your doctor may also check for Murphy’s sign, i.e., asking you to inhale deeply and at the same time press on your liver which will cause a sudden arrest of inhalation due to pain and Boas sign (increased sensitivity to touch).
Other than the above following are some lab investigations to confirm the diagnosis:
Liver function tests (LFTs) are blood tests that assess the health and function of the liver. They measure various components, including liver enzymes (such as ALT and AST), bilirubin levels, Alkaline Phosphatase (ALP), albumin, and total protein, providing insights into liver damage, inflammation, bile duct obstruction, and overall liver function.
Following are some of the differential diagnoses of cholecystitis:
These differentials can be ruled out based on the history given by the patient, the examination performed, and the investigations.
Inflammation of the gallbladder can cause severe complications if left untreated or managed inappropriately. Following are some of the intricacies of Cholecystitis:
Cholecystitis can be managed conservatively in milder forms, i.e., medical management but the definitive treatment in all cases is Cholecystectomy, which involves surgical removal of the gall bladder.
Surgical management includes;
After cholecystectomy, there are several lifestyle changes the patients have to opt for a speedy recovery and reduce future complications. They include:
In cases with no complications or mild to moderate symptoms, it has an excellent recovery rate and very low mortality. On the other hand, the prognosis gets bad in complicated cases, but with the advancement of techniques and instruments, a doctor can prevent complications and manage cholecystitis well.
Our clinical experts continually monitor the health and medical content posted on CURA4U, and we update our blogs and articles when new information becomes available. Last reviewed by Dr.Saad Zia on May 14, 2023.
Acute Cholecystitis - StatPearls - NCBI Bookshelf (nih.gov)
https://www.ncbi.nlm.nih.gov/books/NBK459171/
Acute Cholecystitis: A Review | Surgery | JAMA | JAMA Network
https://jamanetwork.com/journals/jama/article-abstract/2789654




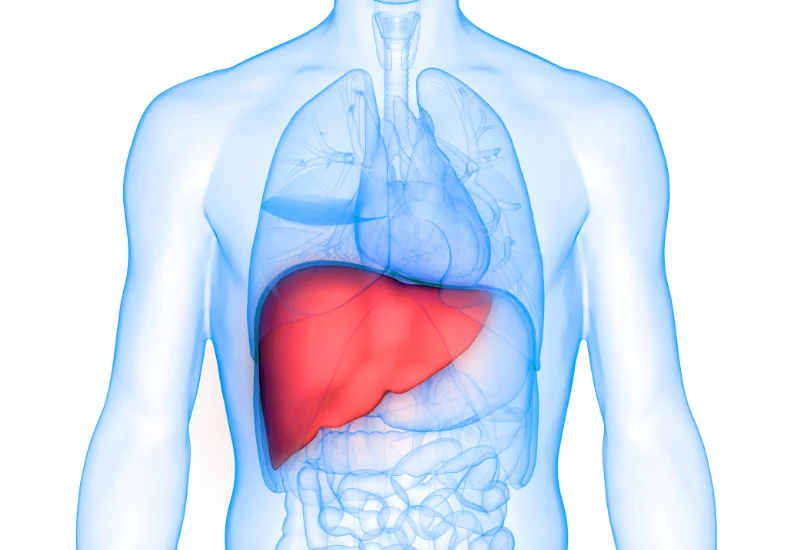
Cholecystitis means inflammation (swelling and redness) of the gallbladder. The gallbladder is a sac attached below the surface of the liver. It is a pear-shaped structure having a body, fundus, neck, and cystic duct. Its primary function is to store “bile,” a greenish fluid produced by the liver and is carried into the gallbladder via the Hepatic duct. Both hepatic and cystic ducts combine to form a Common Bile Duct (CBD) which secretes bile into the small intestine when the food we eat reaches there. The gallbladder releases bile into the Cystic duct, which carries it into the small intestine to digest fats. The gallbladder can typically store about 25-30ml of bitterness. Bile comprises 97% water, bile salts, cholesterol, and bilirubin.